I don’t write many clinical blogs.
Frankly, I don’t even know if I should be writing this blog. In fact I am looking over my shoulder right now. As I write I feel pangs of guilt, shame, and even sometimes anger.
This blog is a response to a year’ s worth of interactions largely on facebook groups, which advocate 3 philosophies:
- Pain science
- Medical research
- An intense hatred of manual therapy
Perhaps the best thing for me to do to try and keep a clear mind is to address these issues in sequence.
The central theme of my blog is a concept called (bet you have had this shoved down your throat since physio met facebook) gulp…
Evidence based practice.
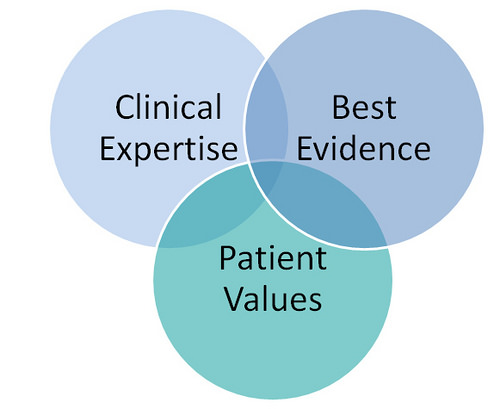
Now firstly, did you know evidence based practice is actually 3 things?
- Evidence from research
- Patient beliefs and preferences AND
- Clinical judgment
A recent paper from esteemed physio ( whom I was lectured by in the early 2000s) Gwen Jull talked about the limitations of evidence based practice, with one of the flaws of the model being the degree to which these 3 components can vary, in the treatment of the same patient, by different practitioners with different philosophies. There is no consistency in the delivery of an evidence based treatment, by a physio, to a patient. In fact, physio is one of the most inconsistent and variable of the medical services. When a patient sees a physio they can get just about any different type of intervention, but generally the goal is the same – education regarding the patient’s condition, a certain level of reduction of pain, and an improvement in movement, function and/or performance.
So patients generally come for the same reasons, but physios deliver a multitude of different services. But is this a bad thing? The other option is we all do the same stuff – and hate our profession, because our ability to use our clinical judgment is being compromised.
I hope that I am writing this blog on behalf of the majority of physios worldwide in private practice who value their many years of experience, which evolves a high level of clinical judgment. I believe this clinical judgment has a high value when treating patients.
Clinical judgment is not worthless – but we are having thoughts jammed down our throat that it is of no value whatsoever – by multiple sources worldwide. Advocates of clinical research do help drive our profession forward and move us away from our old ways, but the old analogy of no RCTs existing for the efficacy of parachutes does ring true with me.
To me clinical judgment is deciding on the best course of action to help a patient. Realistically this clinical judgment may be based on research, patients beliefs, or it may just be based on your experience. At university we were taught that “pattern recognition” when you are treating a patient was evil, and to be avoided like the plague – so why does it seem to work quite often? Aren’t special clinical tests really just a form of pattern recognition? Is this why some clinical tests are less reliable than others? Aren’t the more reliable clinical tests still pattern recognition?
My initial focus is on group 1 – the pain scientists (aka BPS warriors). My main opinions on this topic come from a year’s worth of interaction on the Explain Pain Science facebook page – the purpose of this page at first glance appears to be witch hunts trying to expose practitioners (like me) who believe in a physio’s ability to not miss a biological cause of pain being superior to almost every other health profession, based on our advanced subjective and objective assessment skills. Many of my “friends” on this page would rather skip the assessment and move straight to the counselling. Seek first to understand, my friends. I firmly believe that for pain to have come on, something must have contributed to it coming on – whether it is B, P or S. It can’t be nothing at all – otherwise people who are painfree would have pain as well?? Maybe I have confused myself here.
It may sound petty but sometimes I comment that a problem is entirely biological on this page, just to get a rise out of these people. And my, they are passionate. Passionate about shoving their beliefs down my throat. If I was their patient they are not practising evidence based practice in this situation, as they have failed to consider my beliefs and preferences. There was a post today on the page of an NBA player with a severe tibial fracture, and some members of the group were arguing for the fact that his pain was a complex mesh of biopsychosocial factors. Newsflash guys – the guy just had a compound fracture of a massive friggin’ bone! I mean, get real. I believe it is extremely fashionable at the moment to get on the BPS (read PS) train, and then single out practitioners who do not believe or share your exact beliefs. If there is one thing I have learned, it is not to jam your beliefs down someone’s throat.
The reason the BPS warriors seem so threatening is that they believe they are “the enlightened ones”. Same way as the enlightened ones in the middle aged burned witches at the stake. Same as the enlightened ones in the 1950s prescribed cigarettes for stress. We must all be aware that our clinical beliefs may be proven wrong one day, therefore to be too dogmatic about one’s approach may lead to having a red face in the future.
So let’s talk about group 2 – the researchers. Research is great, until you are in a consult room with a patient with whom you can’t apply any specific research evidence. Consider the person who comes into your consult room, with mild back pain, no history of injury, no medical factors, and some average lifestyle factors – they sit at a desk, they are overweight, they have poor posture (although the researchers may say there is no link between poor posture and pain). Wouldn’t research suggest that we pat these people on the back, with a gentle “there, there” and send them on their way, telling them that their pain is a complex intertwined biopsychosocial mess of adrenalin, cortisol, fear avoidance behaviour, yellow flags, and DIMSIMs.
So researchers – what do we do with people that don’t fit the model? I know where they are – they have been discharged after 1 session by a physio and they are now attending their local chiro 3 times a week for the rest of their life.
I remember a real life example of research vs clinical judgment. Here’s a challenge for you – if a person comes into your clinic with a particular condition, eg patellofemoral pain, and research points towards the need to strengthen a certain muscle, eg VMO, but their VMO tests fine, and other muscles like their hamstring and calf test as weak as water, what do you do? Do you follow your head and strengthen VMO, knowing it’s already functioning pretty well? Or do you follow your heart, knowing you may be cast out of the profession, and strengthen the hamstring or calf? I know what I would do (and have done many, many times). I help the patient strengthen what is weak, not what the textbook tells me I should strengthen for the particular afore mentioned condition.
And finally, group 3 – those with a hatred of manual therapy. Any of us on facebook on a regular basis may have seen some shirts floating around with “manual therapy sucks” on them. Again, this challenges our beliefs when someone comes along and tells us that what we have been taught for 5, 10, 15 or even 20 years “sucks”. I will tell you what doesn’t suck – when you see a patient who can’t life their arm, so you can’t give them any exercises of substance (granted you can give them some simple things to do which will help them) but then as a skilled manual therapist you push on a muscle somewhere, they can move their arm much better, and therefore you can give them better exercises!
Guess what? Deadlifts is not the cure to everything. You can’t push everyone straight into hardcore functional exercise and expect a result, especially if they don’t initially trust you, or their beliefs may need a certain amount of reprogramming. If you hate manual therapy, maybe it is because you have never seen a manual therapist get great results, or you may have tried manual therapy yourself, with limited results? Or someone who hates manual therapy got in your ear.
I don’t just do manual therapy because patients like it – I do it because it helps me get the patients to their goals quickly. I use it in most consultations, and I avoid using it where it is inappropriate. I call this clinical judgment.
So is clinical judgment dead? Who is trying to kill it. The BPS warriors? The researchers? OR the manual therapy haters?
My overall message is this – learn to trust what you have learned to be the best practice for you. Continue to improve and educate yourself, but be wary of people who are particularly dogmatic based on their one approach, as we know patients come in so many shapes, sizes and presentations that one size does truly not fit all, and sometimes a different approach is needed.